We Are Under Construction!
Please check back for updates
Upcoming Workshops
Art of Transformations
Hopi Visit Third Mesa
(Coming Soon 2012)
Art of Transformations
Eden Hot Springs
(Coming Soon 2012)
Articles
HEALTH & BODY
Excerpt from the China Study “Introduction” by T. Collin Campbell, PhD
Enzyme Nutrition: The Food Enzyme Concept by Dr. Edward Howell
Resolving the Coronary Artery Disease Epidemic through Plant-Based Nutrition by Caldwell B. Esselstyn, Jr., MD
NATIVE TRADITIONS
An American Indian Model of the Universe by Benjamin Lee Whorf
Aho Mitakuye Oyasin by Silver Wolf Walks Alone
Ceremony of the Inipi by Black Elk (Excerpted from The Sacred Pipe)
Shamanic Offerings translated by Sara Ñusta
VEDIC TRADITIONS
Gayatri Mantra by Ralph Miller
Agniprasana (Breath of Fire) author unknown
Contact & Subscribe
Art of Transformations
Tunatyava
Linden, Arizona
Please Contact Us to subscribe for updates and additional information.
ReadResolving the Coronary Artery Disease Epidemic through Plant-Based Nutrition
|
 Summary (Abstract)
Summary (Abstract)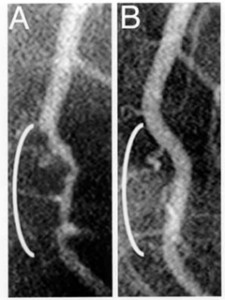 |
Figure 1 -- Coronary angiograms of the distal left anterior descending artery before (left) and after (right) 32 months of a plant-based diet without cholesterol-lowering medication, showing profound improvement. |
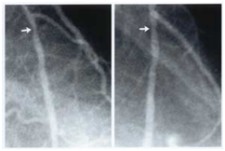 |
Figure 2 -- Coronary angiograms of the circumflex artery before (left) and showing 20% improvement (right) following approximately 60 months of a plant-based diet with cholesterol-lowering medication. |
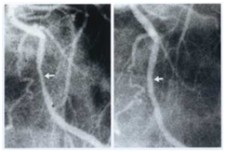 |
Figure 3 -- Coronary angiograms of the proximal left anterior descending artery before (left) and showing 10% improvement (right) following approximately 60 months of a plant-based diet with cholesterol-lowering medication. |
Therapies involving diet and lipid-lowering medication are not ignored by our health-care leaders, but sadly, their recommendations are clearly inadequate. The American Heart Association and the National Cholesterol Education Program (NCEP) recommend consumption of not more than 30% dietary fat and cholesterol levels below 200 mg/dL; numerous studies confirm that people who adhere to these recommendations experience not arrest and reversal of their heart disease, but rather continued disease progression.(16)
A question arises whether these recommendations expose millions to disease development and progression. However, because of the general respect commanded by these organizations, many doctors and patients perhaps are misled, trusting that following their recommendations will protect against heart disease.
"Dr. Scott Grundy, chairman of the NCEP, proclaimed approximately 14 years ago that 90% of heart attacks could be prevented if the population's cholesterol was 150 mg/dL or less."
The newer NCEP clinical guidelines, known as the Adult Treatment Panel 111, suggest broadening the identification of those at risk. This will mandate that millions of Americans take cholesterol-reducing drugs as well as make some dietary and physical activity adjustments. This is a rear-guard, after-the fact approach. It tacitly acknowledges that our food environment is so toxic that millions will become at risk and develop disease. As will be discussed, it is preferable to advise the public to avoid the categories of food that cause atherosclerotic disease.(37)
The National Research Council, in its 1989 report "Diet and Health,"(17) recommended an upper limit of total cholesterol of 200 mg/dL and 30% dietary fat, even though "a number of the scientists felt that a greater reduction would confer additional health benefits."(17) However, the committee felt that setting the cut-off too low would merely frustrate the public. The council also surmised, incorrectly, that if the upper level were set at 200 mg/dL, most Americans would achieve a total cholesterol level of 150 mg/dL or less.(17) That has not happened. Most Americans and their physicians feel "safe" with a cholesterol total of up to 200 mg/dL. They are not. In the Framingham study, 35% of ischemic heart disease occurred in patients with total cholesterol levels between 150 and 200 mg/dL.(18) In the CARE study, the average total cholesterol level in patients with a history of heart attack was 209 mg/dL.(19) In contrast, the American Cancer Society recommends no more than 20% dietary fat,(20) while the World Health Organization prefers no more than 15%.(21)
Dr. Scott Grundy, chairman of the NCEP, proclaimed approximately 14 years ago(22) that 90% of heart attacks could be prevented if the population's cholesterol was 150 mg/dL or less - a figure identical to that hoped for by the National Research Council in 1989. However, neither the NRC, the American Heart Association, or the NCEP is on record to show precisely what diet will achieve the goal of cholesterol of 150 mg/dL. The basic diet favored by these groups contains not only grains, legumes, vegetables, and fruit, but also oil, low-fat milk and milk products, butter, cheese, poultry, lean meat, and fish. I am unaware of any research proving that by eating such a diet one can achieve a cholesterol level of 150 mg/dL or avoid coronary artery disease.
The Mediterranean diet and monounsaturated oils have become unjustifiably popular because of the Lyon Diet Heart Study.(23) This approach is difficult to accept. No studies of monounsaturated oils have shown them to arrest and reverse coronary disease. The Lyon study did show a slower rate of progression, but this is hardly an acceptable goal. In a study of patients with coronary disease, Blankenhorn actually showed the reverse, that disease progressed as rapidly in patients on a monounsaturated diet as it did in those on a saturated fat diet.(24) Rudel demonstrated a similar result in African green monkeys over a 5-year period.(25) Particularly compelling was his finding that disease in the two groups was equivalent, even though the monounsaturated group had higher HDL, lower LDL, and more favorable LDL-to-HDL ratio. He recently replicated the results in rodents.(26)
"Our stop-gap, device-driven, risk factor-oriented approach is not working. Why? Because it fails to address our toxic food environment, which is responsible for the disease."
The number of heart attacks continues to increase every year.(27) Although the age-adjusted death rate for heart disease has declined, the decline may be artifactual.(12) Stamler found deaths from cardiovascular disease approached 40% of those dying in a group of 80,000 young men with follow-up ranging from 16-34 years. The data confirmed a continuous graded relationship of serum cholesterol level to long term risk of coronary heart disease, cardiovascular disease, and all cause mortality. They also demonstrated substantial absolute risk and increased excess risk of coronary heart disease and cardiovascular disease death for younger men with elevated cholesterol levels and conversely a longer estimated life expectancy for younger men with favorable lipids.(35) Our stop-gap, device-driven, risk factor-oriented approach is not working. Why? Because it fails to address our toxic food environment, which is responsible for the disease. It is focused only on those who are already ill or whose elevated lipids reflect an inability to detoxify their American diet. What are the other alternatives?
Taking the Offensive
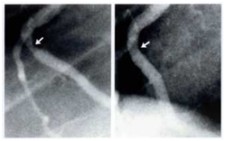 |
Figure 4--Coronary angiograms of right coronary artery before (left) and showing 30% improvement (right) following approximately 60 months of a plant-based diet and cholesterol-lowering medication. |
As I have reported earlier,(28,29) a plant-based diet in conjunction with cholesterol-reducing medication eliminated progression of coronary artery disease over a 12-year period in patients with triple-vessel disease. Most of the 18 patients had experienced an earlier failed intervention of bypass surgery or angioplasty. All patients who maintained the diet achieved the cholesterol goal of less than 150 mg/dL and had no recurrent coronary events during the 12 years. At 5 years, angiography was repeated in most cases. By analysis of the stenosis percentage none had progression of disease, and 70% had selective regression.(28) These data are compelling when one considers that the same group had experienced more than 49 coronary events during the 8 years before this study.(28)
The recent case of a colleague is particularly telling. During September and October of 1996, a 44-year-old surgical colleague experienced occasional chest discomfort, yet neither electrocardiogram, stress echocardiography, or thallium scanning found evidence of disease. While eating the typical American diet, he had a total cholesterol of 156 mg/dL and an LDL of 97 mg/dL. He was lean, non-diabetic, and normotensive, did not smoke, and had no family history of coronary disease. His lipoprotein (a) and homocysteine levels were normal. On November 18, 1996, after his surgical duties, he became acutely ill with pain in the left arm, jaw, and chest. Immediate coronary catheterization found all vessels to be normal except for the left anterior descending artery, the distal third of which was diseased. Enzymes confirmed a myocardial infarction. However, no intervention was deemed appropriate.
This patient was aware of my ongoing study and was curious for more information. He and his wife consulted me for an in-depth review of the plant-based diet and techniques of this arrest and reversal study. He became the personification of commitment to the plant-based diet. Over the next 32 months, without cholesterol-lowering drugs, he maintained a mean total cholesterol of 89 mg/dL and an LDL of 38 mg/dL. The repeat angiogram 32 months after his infarction showed that the disease was completely reversed.(Fig.1)
"Our plant-based diet approach can achieve total disease arrest and selective regression even in advanced cases. This approach is particularly compelling because patients can take control over the disease that was destroying them."
Even though many people might find a plant-based diet initially difficult to follow, every patient with the diagnosis of coronary artery disease should at the least be offered the option of this potentially curative arrest and reversal approach. As this young surgeon's case illustrates, our plant-based diet approach can achieve total disease arrest and selective regression even in advanced cases. This approach is particularly compelling because patients can take control over the disease that was destroying them. If traditional interventional cardiology is a rear-guard action, our arrest and reversal therapy can be likened to a military offensive against atherosclerosis.
Limitations of this study are its modest number of participants and lack of comparable controls. Nevertheless, its size permitted the caregiver an opportunity for frequent patient encounters. These interactions enabled 75% of participants to achieve profound lipid reduction, dietary goals, and relief of symptoms which continued to improve throughout the study's 12-year duration. Patients essentially served as their own controls often achieving profound angiographic reversal of disease as reviewed in the angiographic core laboratory.(Fig. 1-4)
New recommendations for a healthy diet
The expert faculty at the First National Conference on the Elimination and Prevention of Coronary Artery Disease have issued a new set of recommendations:(30)
1) Present nutritional guidelines of government and national health organizations do not provide a maximal opportunity either to arrest or to prevent coronary artery disease.
2) The optimal diet consists of grains, legumes, vegetables, and fruit, with <10%-15% of its calories coming from fat.
This diet minimizes the likelihood of stroke, obesity, hypertension, type II diabetes, and cancers of the breast, prostate, colon, rectum, uterus, and ovary. There are no known adverse effects of such a diet when mineral and vitamin contents are adequate.3) Children and adolescents require major attention to develop early habits of optimal nutrition. Schools should assume a significant leadership role in achieving this goal.
4) Speculation about the degree of public compliance with a low-fat diet must not alter the accuracy of the recommendations.
At the 1999 national cholesterol summit meeting, Dr. William Castelli was asked what he would do to reverse the coronary artery disease epidemic if he were omnipotent. His answer: "Have the public eat the diet of the rural Chinese as described by Dr. T. Colin Campbell," author of the Cornell China study (personal communication, William Castelli, Sept. 2-3, 1999). A recent prospective study of diet quality and mortality in more than 40,000 women confirms the benefits of consuming a diet high in fruits, vegetables, and grains.(31)
At a recent national meeting on hypertension, the original DASH study32 was updated.33 It was found that a diet emphasizing grains, vegetables, and fruit (and including low fat dairy and lean meat), with particular attention to reducing sodium intake, resulted in blood pressure reductions equivalent to those produced by hypertension drugs.(33)
In addition, Dr. Dean Ornish has reported both 1- and 5-year data that support a plant-based approach to control coronary artery disease.16
Replace the "Food Pyramid"
An integral part of this offensive must be to eliminate the toxic food environment. Look at the so-called Food Guide Pyramid, the familiar geometric symbol used to promote the recommendations by the U.S. Department of Agriculture and the Department of Health and Human Services. It is laden with dairy products, animal products, and oils, which are the essential building blocks for coronary artery disease. In addition, from a design standpoint, the choice of a pyramid is potentially confusing and misleading. Some viewers may be led to believe that the foods at the top (meats, sweets, and fatty foods) are the most helpful, when in fact they are the most harmful. To avoid such sources of confusion, we should eliminate geometric figures and promote 3 simple food categories: safe, condiments, and unsafe.
Safe: grains, legumes, lentils, vegetables, and fruits
Condiments: nuts and seeds
Unsafe: oils, dairy foods, meat, poultry, and fish (not regulated by inspection, and frequently contain unacceptable levels of PCB's, dioxin, and mercury)
In addition, we should recommend dietary supplementation with a daily multivitamin, and, for those over 50 years old, an additional 1,000-1,200 mg calcium and 600 to 800 IU of Vitamin D. These recommendations are in concert with those of the expert faculty from the First National Conference on the Elimination of Coronary Artery Disease.(30)
"Any group promoting dietary guidelines for the public should make its decisions based on science. However, the USDA has been subjected to intensive industry lobbying, which compromises its capacity to be fair and objective."
Why are the current recommendations so weak?
When dietary recommendations are issued with the stamp of approval of the U.S. government, the public should be able to trust that these recommendations accurately guide them to foods that are unlikely to cause disease and away from those that are known to cause harm. Thus, any group promoting dietary guidelines for the public should make its decisions based on science. However, the USDA has been subjected to intensive industry lobbying, which compromises its capacity to be fair and objective.(34) At the least, neither the experts who testify before the committee nor the committee members themselves should have relationships, financial or otherwise, to the food industry. These same rules regarding conflict of interest should apply to scientists who lead or are members of the National Cholesterol Education Program and the Food and Nutrition Section of the American Heart Association.
As recently as October, 2000, the Physicians Committee for Responsible Medicine successfully litigated the USDA to ascertain the compensation sources of the US Dietary Guidelines Committee. Six of the eleven committee members, including the chairman, had relationships to the meat, dairy, or egg industry.(36) Such conflict insures a perception that the American public and school children will not receive an unbiased recommendation of what constitutes the healthiest food choices. The USDA, by definition, a protector of the agriculture industry should disqualify itself from this responsibility, which more correctly may belong in the Centers for Disease Control.
Summary
The present device-driven, risk factor-identification, rear-guard strategy diagnoses disease after the fact and offers no promise of preventing disease or controlling its progression. We are fortunate to possess the knowledge of how to prevent, arrest, and selectively reverse this disease. However, we are not fortunate in the capacity of our institutions to share this information with the public. The collective conscience and will of our profession is being tested as never before. Ties to industry and politics result in conflict within our private and governmental health institutions, compromising the accuracy of their public message. This is in total violation of the moral imperative of our profession. The time is now for us to have the courage for legendary work. Science and not the messenger must dictate the recommendations.
References
1) Braunwald E. Shattuck Lecture: Cardiovascular medicine at the turn of the millennium: triumphs, concerns and opportunities. N Engl J Med 1997;337:1360-69.
2) Enos WF, Holmes RH, Beyer J. Coronary disease among United States soldiers killed in action in Korea. JAMA 1953;152:1090-1093.
3) McNamara JJ, Molot MA, Stremple JF, Cutting RT. Coronary artery disease in combat casualties in Vietnam. JAMA 1971;216:1185-1187.
4) Berenson G, Srinivasan S, Bau W, Newman WP, Tracy RE, Wattingney WA. Association between multiple cardiovascular risk factors and atherosclerosis in children and young adults. N Engl J Med 1998;338:1650-1656.
5) Strong JP, Malcolm GT, McMahan C, Tracy R, Newman W, Hederick E, Cornhill J. Prevalence and extent of atherosclerosis in adolescents and young adults. JAMA 1999;281:727-735.
6) Ziada KM, Kapadia SR, Tuzcu EM, Nissen SE. The current status of intravascular ultrasound imaging. Curr Probl Cardiol 1999 Sept;24 (9):541-66.
7) Roberts WC. Coronary atherosclerosis: Is the process focal or diffuse among patients with symptomatic or fatal myocardial ischemia. Am J Card 1998; 82(10B):41T-44T.
8) Connor WE, Cerqueira MT, Connor RW, et al. The plasma lipids, lipoproteins, and diet of the Tarahumara Indians of Mexico. Am J Clin Nutr 1978;31:1131-42.
9) Sinnett PF, Whyte HM. Epidemiological studies in a total highland population, Tukisenta, New Guinea. Cardiovascular disease and relevant clinical, electrocardiographic, radiological and biochemical findings. J Chron Diseases 1973; 26:265.
10) Campbell TC, Parpia B, Chen J. Diet, lifestyle, and the etiology of coronary artery disease: The Cornell China Study. Am J Card 1998;82(10B):18T-21T.
11) Miller K. Lipid values in Kalahari Bushman. Arch Intern Med 1968; 121:414.
12) Breslow JL. Cardiovascular disease myths and facts. Cleve Clin J Med 1998; 65(6):286-287.
13) The Bypass Angioplasty Revascularization Investigation (BARI) Investigators. Comparison of coronary bypass surgery with angioplasty in patients with multivessel disease. N Engl J Med 1996;335:217-225.
14) Ambrose JA, Fuster V. Can we predict future coronary events in patients with stable coronary artery disease? JAMA 1997;277:343-344.
15) Forrester JS, Shah PK. Lipid lowering versus revascularization - an idea whose time for testing has come. Circulation 1997;96:1360-1362.
16) Ornish D, Scherwitz LW, Billings JH, Gould KL, Merritt TA, Sparler S, Armstrong WT, Ports TA, Kirkeeide RL, Hogeboom C, Brand RJ. Intensive lifestyle changes for reversal of coronary heart disease. JAMA 1998;280:2001-2007.
17) National Research Council (US) Committee on Diet & Health. Diet and health: implications for reducing chronic disease risk/Committee on Diet and Health, Food and Nutrition Board, Commission on Life Sciences; National Research Council. Washington, DC: National Academy Press, 1989.
18) Castelli W. Take this letter to your doctor. Prevention 1996;48:61-64.
19) Sacks FM, Pfeffer MA, Moye LA, Rouleau JL, Rutherford JD, Cole TG, Brown L, Warnica JW, Arnold JMO, Wun C, Davis BR, Braunwald E. The effect of pravastatin on coronary events after MI in patients with average cholesterol levels. N Engl J Med 1996;335:1001-1009.
20) The American Cancer Society 1996 Advisory Committee on Diet, Nutrition, and Cancer Prevention. Guidelines on diet, nutrition, and cancer prevention: reducing the risk of cancer with healthy food choices and physical activity. CA Cancer J Clin 1996;46:325-341.
21) WHO study group in diet, nutrition, and prevention of non-communicable diseases. Diet, nutrition and the prevention of chronic diseases: report of a WHO study group. WHO Technical Report Series 1990:797.
22) Elias M. Doctors get guidelines for healthy heart. USA Today 1987 June 9;Final Edition-News:01A.
23) de Lorgeril M, Salen P, Martin JL, Monjaud I, Deloye J, Mamelle N. Mediterranean diet, traditional risk factors, and the rate of cardiovascular complications after myocardial infarction. Circulation 1999;99:779-785.
24) Blankenhorn DH, Johnson RL, Mack WJ, El Zein HA, Vailas LI. The influence of diet on the appearance of new lesions in human coronary arteries. JAMA 1990;263(12):1646-1652.
25) Rudel LL, Parks JS, Sawyer JK. Compared with dietary monounsaturated and saturated fat, polyunsaturated fat protects African Green Monkeys from coronary artery atherosclerosis. Arterioscler Thromb Vasc Biol 1995;15:2101- 2110.
26) Rudel LL, Kelley K, Sawyer JK, Shah R, Wilson MD. Dietary monounsaturated fatty acids promote aortic atherosclerosis in LDL receptor-Null, human ApoB100-overexpressing transgenic mice. Arterioscler Thromb Vasc Biol 1998;18(11): 1818-1827.
27) Rosamond WD, Chambless LE, Folsom AR, Cooper LS, Conwill DE, Clegg L, Wang,CH, Heiss, G. Trends in the incidence of myocardial infarction and in mortality due to coronary heart disease, 1987 to 1994. N Eng J Med 1998; 339(13):861-867.
28) Esselstyn CB Jr, Ellis SG, Medendorp SV, Crowe TD. A strategy to arrest and reverse coronary artery disease: a 5-year longitudinal study of a single physician's practice. J Fam Prac 1995;41:560-568.
29) Esselstyn CB Jr. Updating a 12-year experience with arrest and reversal therapy for coronary heart disease (An overdue requiem for palliative cardiology). Am J Card 1999;84:339-341.
30) Esselstyn CB Jr. Foreword: Changing the treatment paradigm for coronary artery disease. Am J Card 1998;82(10B):2T-4T.
31) Kant AK, Schatzkin A, Graubard BI, Schairer C. A prospective study of diet quality and mortality in women. JAMA 2000;283(16):2109-2115.
32) Appel LJ, Moore TJ, Orbarzanek E, Vollmer WM, Svetkey LP, Sacks FM, Bray GA, Vogt TM, Cutler JA, Windhauser MM, Lin PH, Karanja N. A clinical trial of the effects of dietary patterns on blood pressure. N Engl J Med 1997;336:1117- 1124.
33) Grady D. Low-salt and high-produce diet is found to tame hypertension. The New York Times 2000 May 18;National:A19.
34) Radetsky P. The Live Longer Diet. Why doesn't the government want you to eat it? Longevity Magazine 1994 May:40.
35) Stamler J, Daviglus ML, Garside DB, Dyer AR, Greenland P, Neaton JD. Relationship of baseline serum cholesterol levels in 3 large cohorts of younger men to long-term coronary, cardiovascular, and all-cause mortality and to longevity. JAMA 2000 July 19;284(3):311-318.
36. Personal communication 12/21/2000 with Dr. Neal Barnard, Chairman of the Physicians Committee for Responsible Medicine.
37. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults ( Adult Treatment Panel 111) Executive Summary of the Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel 111). JAMA. 2001; 285; 2486-2497.
Fig. 1. Coronary angiograms of distal left anterior descending artery before (left) and showing profound improvement (right) following 32 months of a plant-based diet without cholesterol-lowering medication.
Fig. 2. Coronary angiograms of proximal left anterior descending before (left) and showing 10% improvement (right) following approximately 60 months of a plant-based diet with cholesterol-lowering medication.
Fig. 3. Coronary angiograms of circumflex artery before (left) and showing 20% improvement (right) following approximately 60 months of a plant-based diet with cholesterol-lowering medication.
Fig. 4. Coronary angiograms of right coronary artery before (left) and showing 30% improvement (right) following approximately 60 months of a plant-based diet and cholesterol-lowering medication.
© Art of Transformations 2012
